5 thoughts on “Therapies for cognitive impairment in breast cancer patients associated with chemotherapy: A meta analysis”
Hi Sababa,
Nice work. Please see my comments and questions below:
Comments:
(1) In your conclusion, you reference Fig. 1 where I think you mean Fig. 2.
Questions:
(1) How can we know that the combined effect size observed across the seven CBT studies is more than we would expect to have found by chance alone in a world where there really is no effect of CBT? In other words, how would you go about reaching a statistical conclusion about the combined CBT effect size?
(2) A major objective of the study was to compare efficacy across intervention types. Do you think that is possible, given the number of studies included in the current meta-analysis? Are there ways to increase the rate at which you capture studies that meet your inclusion/exclusion criteria?
Thank you for your feedback and for noticing the mis-referenced figures!
As for your questions:
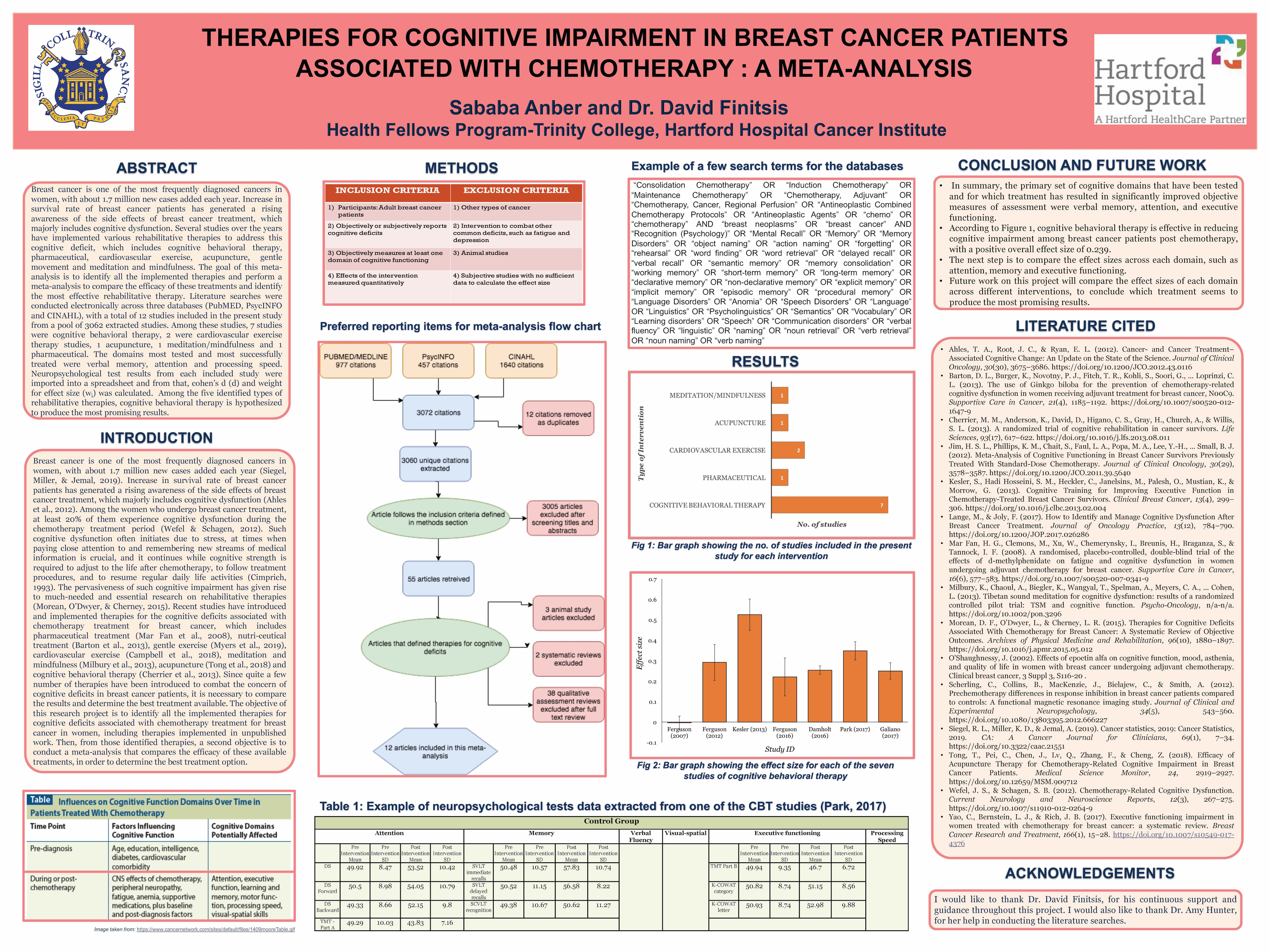
From the values of mean and standard deviation for each neuropsychological test, effect sizes and the confidence intervals were calculated, first manually with an excel spreadsheet, and then was further cross-checked with the software, R. Out of the 12 included studies, seven studies were for cognitive behavioral therapy, which was very high compared to the other types of interventions. Since comparing across interventions would not be very effective due to a large difference in the number of studies, we decided to look more closely at cognitive behavioral therapy instead (as time was limited to complete this project). The effect size of 0.239 represented the average effect on every domain all lumped together, hence we later decided to split the effect by neurocognitive domains (which is not included in the poster, as the poster had to be printed ahead of time). The results from that showed that Cognitive Behavioral Therapy (CBT) has no significant effect on most domains studied, except for memory. It was also interesting to note that the neurocognitive domain with the largest number of studies, memory (k=6), also had the highest and only significant observed effect. Hence this could perhaps lead to a conclusion that cognitive behavioral therapy is a valuable treatment for patients complaining of memory decrements after cancer treatment.
This review was limited by having only included articles that reported objective neuropsychological measures of cognitive performance. Articles that strictly reported subjective measurement outcomes of treatments were not included. The review was also restricted by time, as it was a semester long research project and article screening took a significant portion of the allocated time. Besides that, we couldn’t include a few articles even though they fit the inclusion/exclusion criteria, as we had reached out the authors for more information on data tables but we didn’t get a promising response from them. Moreover, there was a great deal of heterogeneity present in the populations studied, such as cancer types, treatment type, the length of time they were studied for, and the tests used to measure cognitive function. All these factors challenge the goal of precise estimation and adds error to the overall picture. There is however, considerable room for future research on other types of interventions, which could be helpful for future meta-analysis that compares the effect sizes across interventions.
Thank you for your responses. There is indeed a way to statistically determine if that average effect size across all CBT studies is reliably different than 0, in other words to determine if chance alone accounts for the fact that the average effect size is 0.239. Without going into too much detail, you can determine the variance in your effect sizes across studies, then use this to construct a 95% confidence interval around the mean effect size value that you report. If that interval overlaps with 0, then you would conclude that CBT interventions really don’t have a reliably positive impact on cognitive function (the reverse would be true if it doesn’t overlap with 0). Just an FYI.
Hello Sababa,
Well done with your research. It was very interesting to learn about the complications that present after a patient goes through treatment for cancer. It really shows how stress can become an illness of its own.
The only questions I have about your research are, How did you compare the research you found in order to see which treatment method was more effective? How did the fact that all research experiments use different variables and size experimental groups affect your statistical analysis?
The necessary information from the studies were first extracted into the coding forms, then were transferred to an excel spreadsheet. From the values of mean and standard deviation for each neuropsychological test, effect sizes and the confidence intervals were calculated, first manually with an excel spreadsheet, and then was further cross-checked with the software, R. Across the twelve articles, over thirty different neuropsychological tests were used to measure cognitive function objectively. Among those, seven tests were repeated across studies, which included High Sensitivity Cognitive Screen, Trail Making test (TMT-A and TMT-B), Stroop Test, Hopkins Verbal Learning Test (HVLT), California Verbal Learning Test, Digit Symbol Coding and Digit Span (Table 1). Besides that, the most tested cognitive domains were attention, memory and processing speed. As per the results shown in Figure 1, cognitive behavioral therapy had the most number of studies, so instead of looking at effect sizes across different types of interventions, we decided to look more closely at cognitive behavioral therapy (due to time restrictions). This led to a new research question, of whether cognitive behavioral interventions (CBT) is efficacious in treatment of cancer related cognitive impairment (CRCI). The effect size of 0.239 in CBT represented the average effect on every domain all lumped together, hence we later decided to split the effect by neurocognitive domains (which is not included in the poster, as the poster had to be printed ahead of time). The results from that showed that Cognitive Behavioral Therapy (CBT) has no significant effect on most domains studied, except for memory. It was also interesting to note that the neurocognitive domain with the largest number of studies, memory (k=6), also had the highest and only significant observed effect. Hence this could perhaps lead to a conclusion that cognitive behavioral therapy is a valuable treatment for patients complaining of memory decrements after cancer treatment.

Hi Sababa,
Nice work. Please see my comments and questions below:
Comments:
(1) In your conclusion, you reference Fig. 1 where I think you mean Fig. 2.
Questions:
(1) How can we know that the combined effect size observed across the seven CBT studies is more than we would expect to have found by chance alone in a world where there really is no effect of CBT? In other words, how would you go about reaching a statistical conclusion about the combined CBT effect size?
(2) A major objective of the study was to compare efficacy across intervention types. Do you think that is possible, given the number of studies included in the current meta-analysis? Are there ways to increase the rate at which you capture studies that meet your inclusion/exclusion criteria?
Hi Professor Martinez,
Thank you for your feedback and for noticing the mis-referenced figures!
As for your questions:
From the values of mean and standard deviation for each neuropsychological test, effect sizes and the confidence intervals were calculated, first manually with an excel spreadsheet, and then was further cross-checked with the software, R. Out of the 12 included studies, seven studies were for cognitive behavioral therapy, which was very high compared to the other types of interventions. Since comparing across interventions would not be very effective due to a large difference in the number of studies, we decided to look more closely at cognitive behavioral therapy instead (as time was limited to complete this project). The effect size of 0.239 represented the average effect on every domain all lumped together, hence we later decided to split the effect by neurocognitive domains (which is not included in the poster, as the poster had to be printed ahead of time). The results from that showed that Cognitive Behavioral Therapy (CBT) has no significant effect on most domains studied, except for memory. It was also interesting to note that the neurocognitive domain with the largest number of studies, memory (k=6), also had the highest and only significant observed effect. Hence this could perhaps lead to a conclusion that cognitive behavioral therapy is a valuable treatment for patients complaining of memory decrements after cancer treatment.
This review was limited by having only included articles that reported objective neuropsychological measures of cognitive performance. Articles that strictly reported subjective measurement outcomes of treatments were not included. The review was also restricted by time, as it was a semester long research project and article screening took a significant portion of the allocated time. Besides that, we couldn’t include a few articles even though they fit the inclusion/exclusion criteria, as we had reached out the authors for more information on data tables but we didn’t get a promising response from them. Moreover, there was a great deal of heterogeneity present in the populations studied, such as cancer types, treatment type, the length of time they were studied for, and the tests used to measure cognitive function. All these factors challenge the goal of precise estimation and adds error to the overall picture. There is however, considerable room for future research on other types of interventions, which could be helpful for future meta-analysis that compares the effect sizes across interventions.
Hi Sababa,
Thank you for your responses. There is indeed a way to statistically determine if that average effect size across all CBT studies is reliably different than 0, in other words to determine if chance alone accounts for the fact that the average effect size is 0.239. Without going into too much detail, you can determine the variance in your effect sizes across studies, then use this to construct a 95% confidence interval around the mean effect size value that you report. If that interval overlaps with 0, then you would conclude that CBT interventions really don’t have a reliably positive impact on cognitive function (the reverse would be true if it doesn’t overlap with 0). Just an FYI.
Best,
Prof. Martinez
Hello Sababa,
Well done with your research. It was very interesting to learn about the complications that present after a patient goes through treatment for cancer. It really shows how stress can become an illness of its own.
The only questions I have about your research are, How did you compare the research you found in order to see which treatment method was more effective? How did the fact that all research experiments use different variables and size experimental groups affect your statistical analysis?
Hi Anes,
Thank you for your feedback!
The necessary information from the studies were first extracted into the coding forms, then were transferred to an excel spreadsheet. From the values of mean and standard deviation for each neuropsychological test, effect sizes and the confidence intervals were calculated, first manually with an excel spreadsheet, and then was further cross-checked with the software, R. Across the twelve articles, over thirty different neuropsychological tests were used to measure cognitive function objectively. Among those, seven tests were repeated across studies, which included High Sensitivity Cognitive Screen, Trail Making test (TMT-A and TMT-B), Stroop Test, Hopkins Verbal Learning Test (HVLT), California Verbal Learning Test, Digit Symbol Coding and Digit Span (Table 1). Besides that, the most tested cognitive domains were attention, memory and processing speed. As per the results shown in Figure 1, cognitive behavioral therapy had the most number of studies, so instead of looking at effect sizes across different types of interventions, we decided to look more closely at cognitive behavioral therapy (due to time restrictions). This led to a new research question, of whether cognitive behavioral interventions (CBT) is efficacious in treatment of cancer related cognitive impairment (CRCI). The effect size of 0.239 in CBT represented the average effect on every domain all lumped together, hence we later decided to split the effect by neurocognitive domains (which is not included in the poster, as the poster had to be printed ahead of time). The results from that showed that Cognitive Behavioral Therapy (CBT) has no significant effect on most domains studied, except for memory. It was also interesting to note that the neurocognitive domain with the largest number of studies, memory (k=6), also had the highest and only significant observed effect. Hence this could perhaps lead to a conclusion that cognitive behavioral therapy is a valuable treatment for patients complaining of memory decrements after cancer treatment.